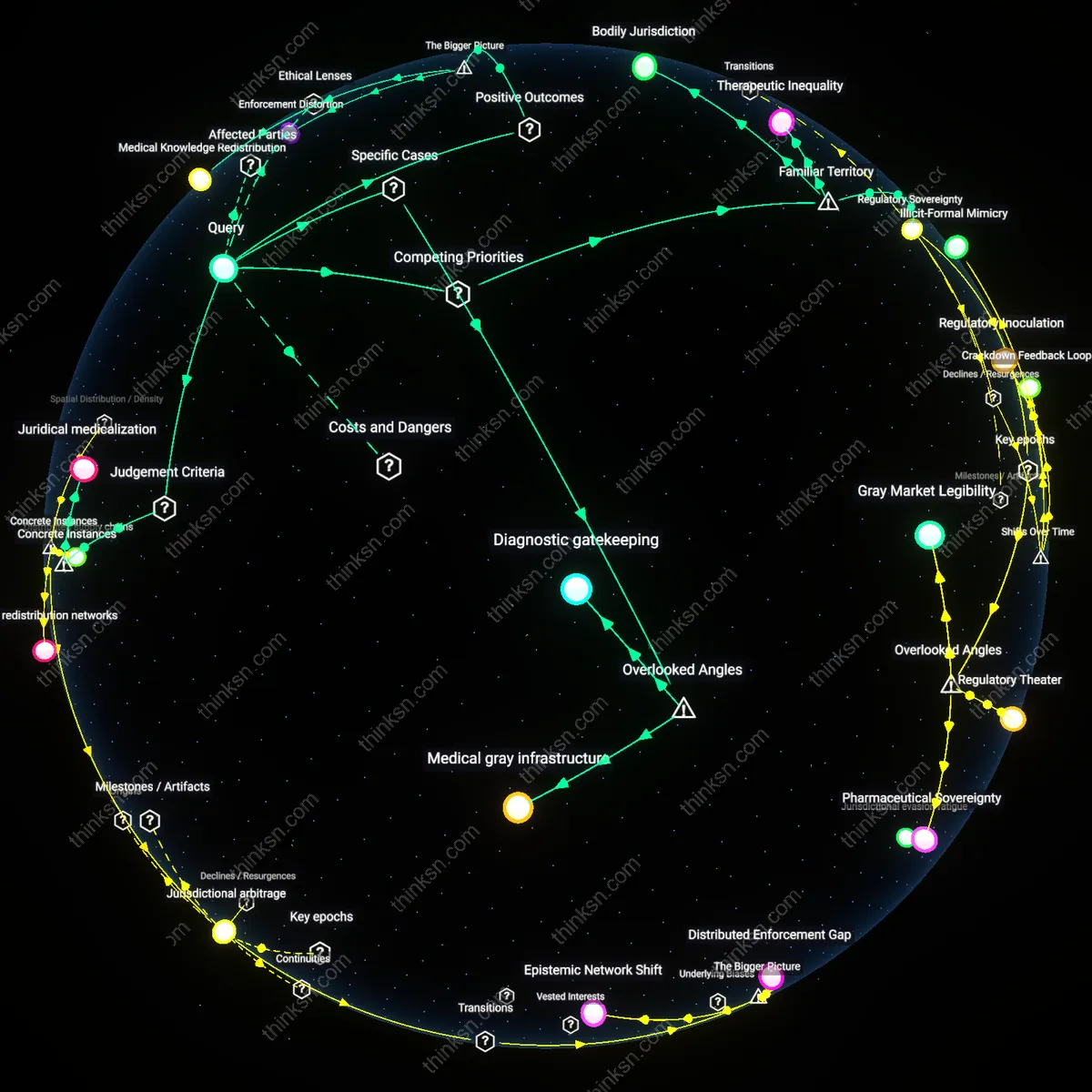
Patent Override in Crisis: Balancing Lives and Innovation?
Analysis reveals 6 key thematic connections.
Key Findings
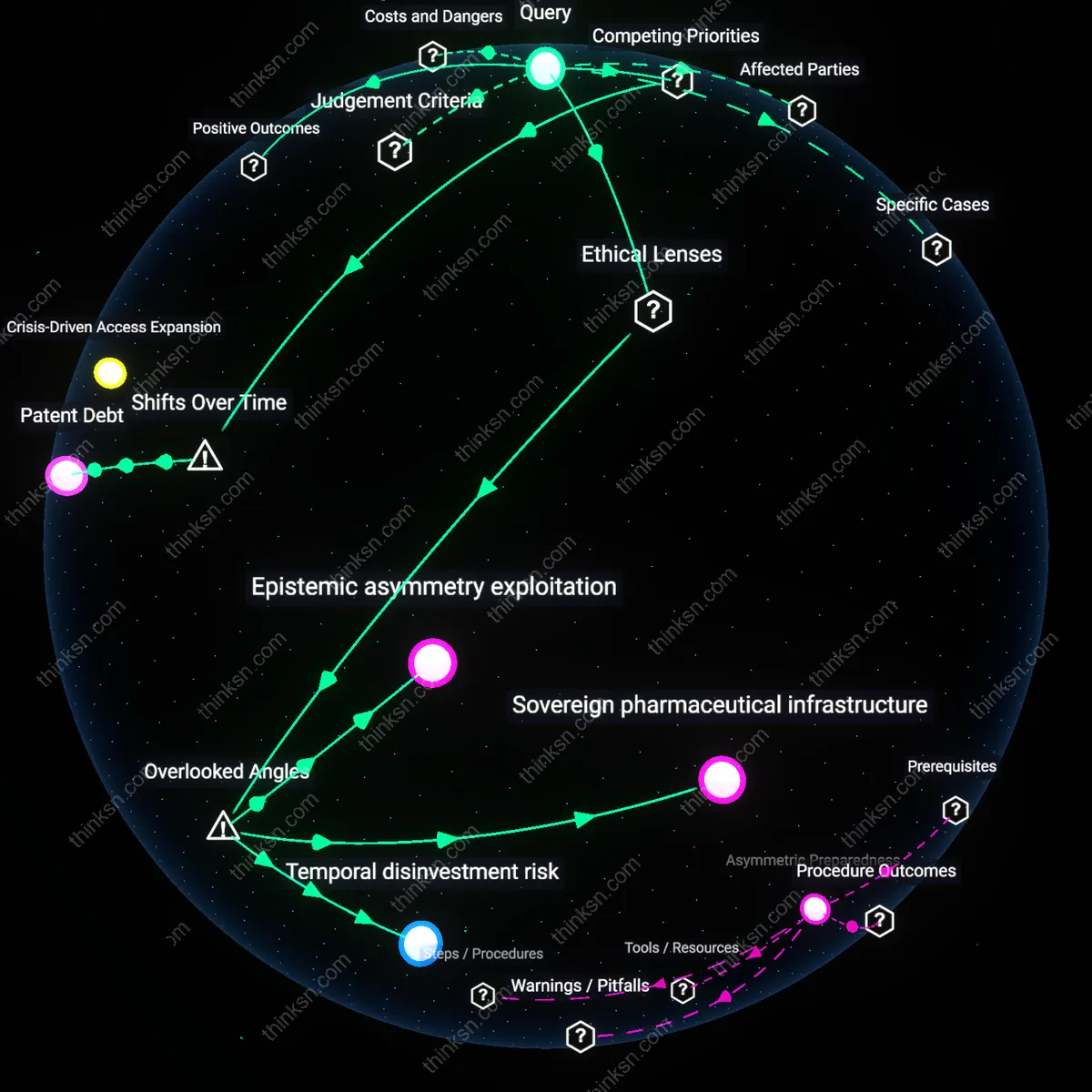
Crisis-Driven Access Expansion
Governments using compulsory licensing during public health emergencies directly expand access to life-saving drugs by overriding patent barriers, enabling rapid production of generics through domestic manufacturers. This mechanism is activated by acute demand-supply imbalances during epidemics, where pharmaceutical firms cannot scale output quickly enough, and it operates through state authority to invoke WTO-trips flexibilities, as seen in Thailand’s 2006 HIV drug licensing. The non-obvious systemic effect is that the threat of compulsory licensing recalibrates pharmaceutical pricing strategies in anticipation of future emergencies, enhancing long-term access even without invocation.
Global Health Norm Contagion
The use of compulsory licensing by one nation during a health emergency strengthens the legitimacy of similar actions globally by reinforcing norms of health as a human right over strict IP enforcement, as demonstrated when Brazil and South Africa challenged antiretroviral patents in the early 2000s. This normative shift spreads through transnational advocacy networks, international courts, and WTO dispute settlements, altering the behavior of both governments and the pharmaceutical industry by raising reputational costs for blocking access. The systemic consequence is a self-reinforcing precedent where emergency licensing becomes institutionally expected, not exceptional—thus embedding equity into global health governance structures.
Patent Debt
The ethical justification for compulsory licensing has evolved since the 2010s because the financialized pharmaceutical model—where R&D is increasingly funded by speculative capital and pricing power, not public grants—has created a moral ledger where firms extract monopolistic rents in peacetime, generating a reciprocal obligation to relinquish those rents during emergencies. This shift from public-interest-driven patenting to shareholder-driven pricing, exemplified by post-2010 insulin and hepatitis C drug controversies, reframes access during crises not as a threat to innovation but as the repayment of a distributive debt accrued through years of unencumbered profit extraction. The underappreciated dynamic is that compulsory licensing now functions as a corrective mechanism within a longer arc of equity claims, revealing that patent rights are increasingly seen as contingent on social reinvestment.
Epistemic asymmetry exploitation
Yes, because governments leveraging compulsory licensing during health crises expose and correct an underacknowledged epistemic asymmetry where pharmaceutical firms withhold real-world clinical utility data under patent protection, thus impeding socially optimal treatment scaling; this dynamic reveals that innovation is not solely about molecule creation but also about knowledge distribution, a factor typically absent in innovation incentive debates. Most analyses assume patents are necessary to incentivize R&D investment, yet they overlook how patent regimes also institutionalize information hoarding, which compulsory licensing disrupts by forcing data transparency through state-backed use, thereby recalibrating the innovation ecosystem toward collective learning rather than proprietary accumulation. This shifts the ethical burden from rewarding past innovation to enabling future adaptation, a transformation rarely captured in utilitarian or deontological drug access frameworks.
Sovereign pharmaceutical infrastructure
Yes, because compulsory licensing activates latent state capacity in countries with existing but underutilized domestic manufacturing capabilities—such as India’s generic drug plants or South Africa’s formulation facilities—transforming them into instruments of health sovereignty during emergencies; this reframes the debate away from charity or IP violation toward the strategic reconstruction of pharmaceutical self-reliance as a public good. Standard discussions treat compulsory licensing as a temporary override of global IP rules, missing how repeated use builds material and institutional infrastructure that diminishes long-term dependency on multinational drug suppliers, thereby altering the balance of power in global health governance. This transformation is a slow, structural consequence often invisible in short-term innovation incentive models, which fail to account for distributed production networks as ethical assets.
Temporal disinvestment risk
No, because the justified use of compulsory licensing inadvertently accelerates a temporal disinvestment risk where venture capital and biotech startups shift focus from long-tail therapeutic platforms—like broad-spectrum antivirals or pandemic preparedness tools—toward narrow, rapidly monetizable diagnostics or lifestyle drugs that avoid exposure to state appropriation during crises; this effect bypasses headline innovation metrics but erodes foundational research pipelines in preemptive medicine. While ethical frameworks emphasize access during emergencies, they rarely consider how licensing unpredictability skews the time horizon of private investment, privileging speed-to-market over sustained scientific resilience. This hidden time preference distortion undermines the very innovation needed for future emergencies, revealing a feedback loop between emergency policy and pre-crisis research neglect.