Regulatory Threshold Drift
The 1992 accelerated approval of misoprostol for gastric ulcers under FDA Commissioner David Kessler marked a pivotal shift, where benefit thresholds were lowered due to pressure from gastroenterologists and pharmaceutical sponsors amidst rising ulcer-related hospitalizations. The mechanism was a pragmatic relaxation of efficacy standards—accepting surrogate endpoints like endoscopic ulcer reduction rather than clinical symptom relief—established through informal negotiation between the FDA’s Division of Gastroenterological Drug Products and Searle’s clinical teams. This case reveals the underappreciated process by which emergency authorization frameworks, initially designed for life-threatening conditions, migrate into chronic disease domains, normalizing incremental benefit acceptance.
Regulatory Epistemic Drift
Drug approval norms shifted because regulatory agencies gradually accepted weaker evidence thresholds as standard when faced with political and industrial pressure to accelerate access, a change that was rarely formalized but embedded through successive guidance documents and precedent-setting case reviews at the FDA and EMA. Internal review memos and advisory committee records show that incremental decisions—such as allowing smaller trials or surrogate endpoints in oncology or metabolic diseases—normalized marginal efficacy by redefining what counted as a ‘meaningful’ benefit, particularly when patient advocacy groups framed access as an ethical imperative. This dynamic is overlooked because most analyses focus on explicit policy changes or corruption, not the slow transformation of evidentiary standards within expert communities; what matters is that the bar for proof eroded not through overt repeal but through accumulated administrative precedent. The consequence is a system where marginal benefit is not an exception but the calibrated outcome of evolved interpretation.
Therapeutic Index Gaming
Pharmaceutical developers learned to manipulate the structure of clinical trial design by narrowly targeting patient subpopulations or using composite endpoints where a single positive component could justify approval, even if net clinical benefit was negligible, a practice refined in the 1990s biotech era through statistical arbitrage rather than therapeutic breakthrough. Firms like those in the late-1990s cardiovascular drug space demonstrated that splitting endpoints across morbidity markers allowed drugs to ‘succeed’ on secondary outcomes while failing primary ones, yet still gain approval due to regulatory reluctance to reject on technical grounds. This gaming is rarely highlighted in public discourse, which assumes trials measure holistic patient outcomes, not that companies exploit the multiplicity of measurable indices to manufacture significance; the real mechanism is not fraud but strategic alignment of trial architecture with regulatory blind spots. The result is a system where marginality is not accidental but engineered into the metrics themselves.
Reimbursement Contingency Alignment
Health technology assessment bodies in countries like Germany and the UK inadvertently enabled marginal approvals by decoupling initial marketing authorization from post-market pricing negotiations, creating a financial incentive for manufacturers to pursue even minimally effective drugs knowing that payers would later absorb evaluation through separate cost-effectiveness reviews. The AMNOG law in Germany, for instance, guarantees temporary market access before benefit assessment, allowing firms to commercialize drugs with unproven added benefit while negotiating reimbursement levels retroactively, thus making marginal efficacy a viable business model. This structural misalignment between approval and payment is typically ignored in U.S.-centric critiques that conflate FDA and payer roles, obscuring how segmented decision architectures enable low-efficacy drugs to flourish in regulated markets. The key insight is that marginality becomes routine not because regulators lower standards, but because systems distribute accountability across non-overlapping institutional mandates.
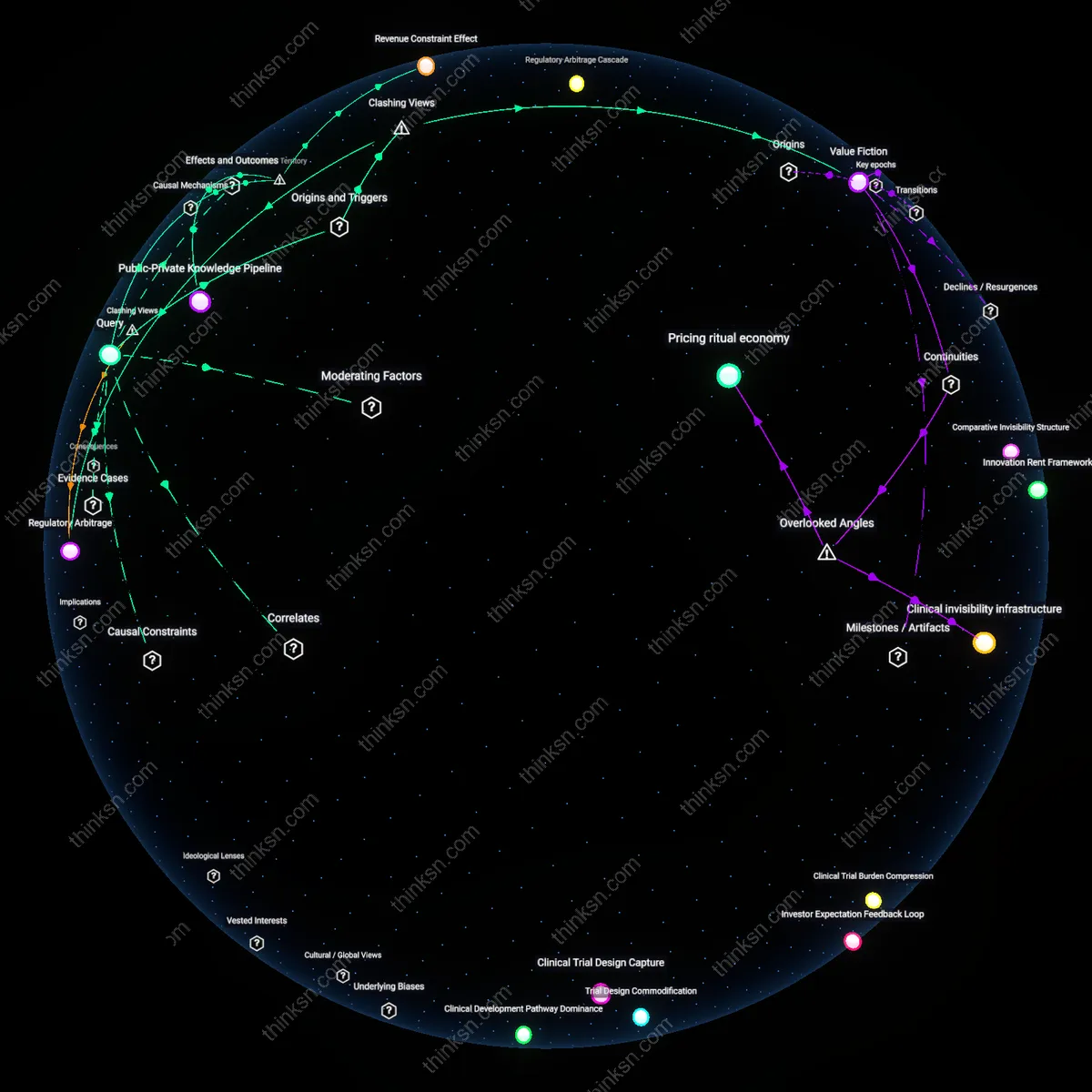
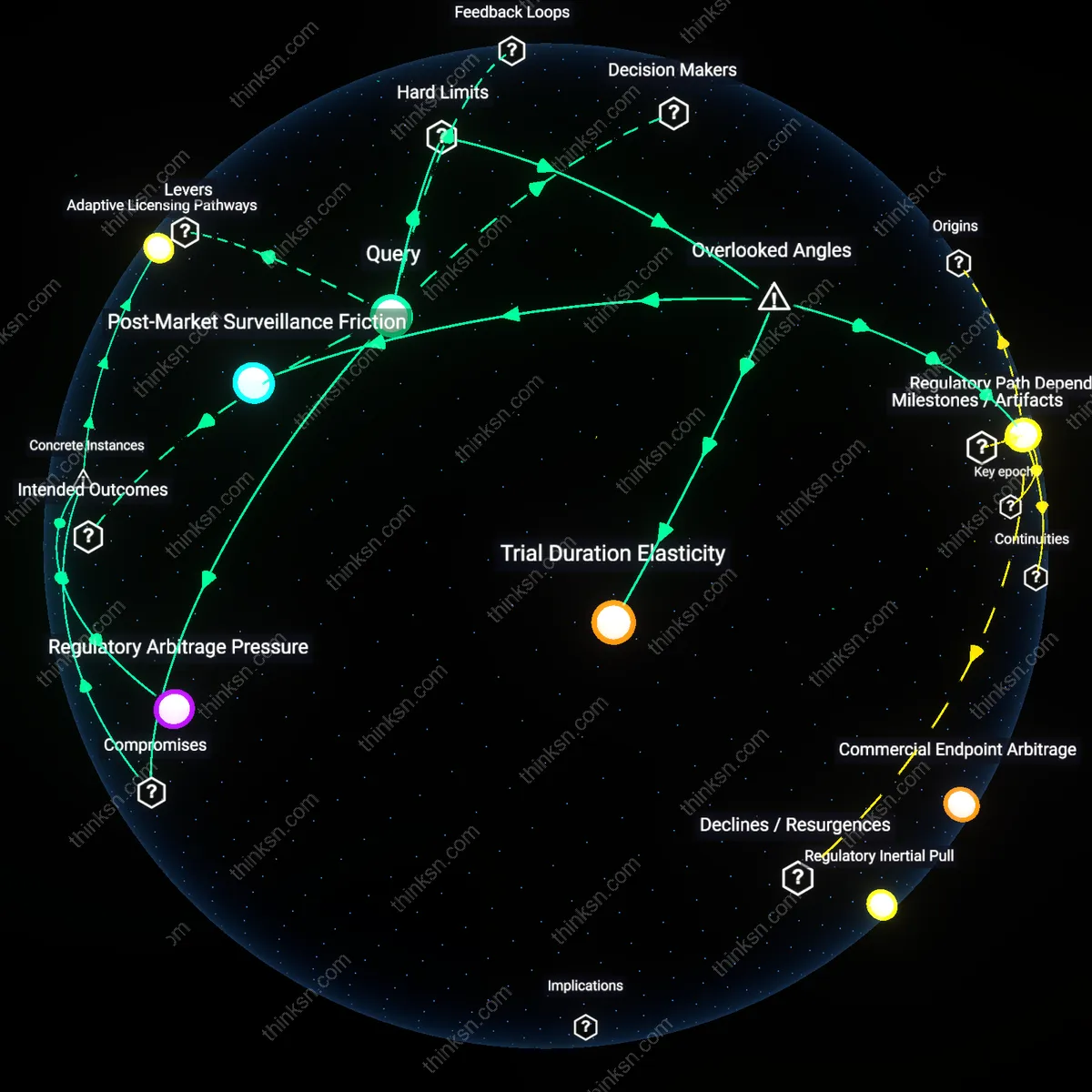
Regulatory Arbitrage
The routinization of marginal-benefit drug approvals emerged when regulatory agencies began treating statistical significance as a proxy for clinical meaningfulness, allowing pharmaceutical sponsors to exploit endpoint selection and trial design to meet approval thresholds without demonstrating patient-relevant outcomes. This shift, cemented in the 1980s with the adoption of surrogate markers in diseases like hypertension and hyperlipidemia, decoupled approval from therapeutic impact by institutionalizing a mechanistic interpretation of efficacy—one that prioritized reproducible biomarker shifts over functional improvement. The non-obvious insight is that agencies did not lower standards so much as redefine compliance, enabling firms to game the criteria through design rather than fraud, thus normalizing drugs with benefits invisible at the bedside.
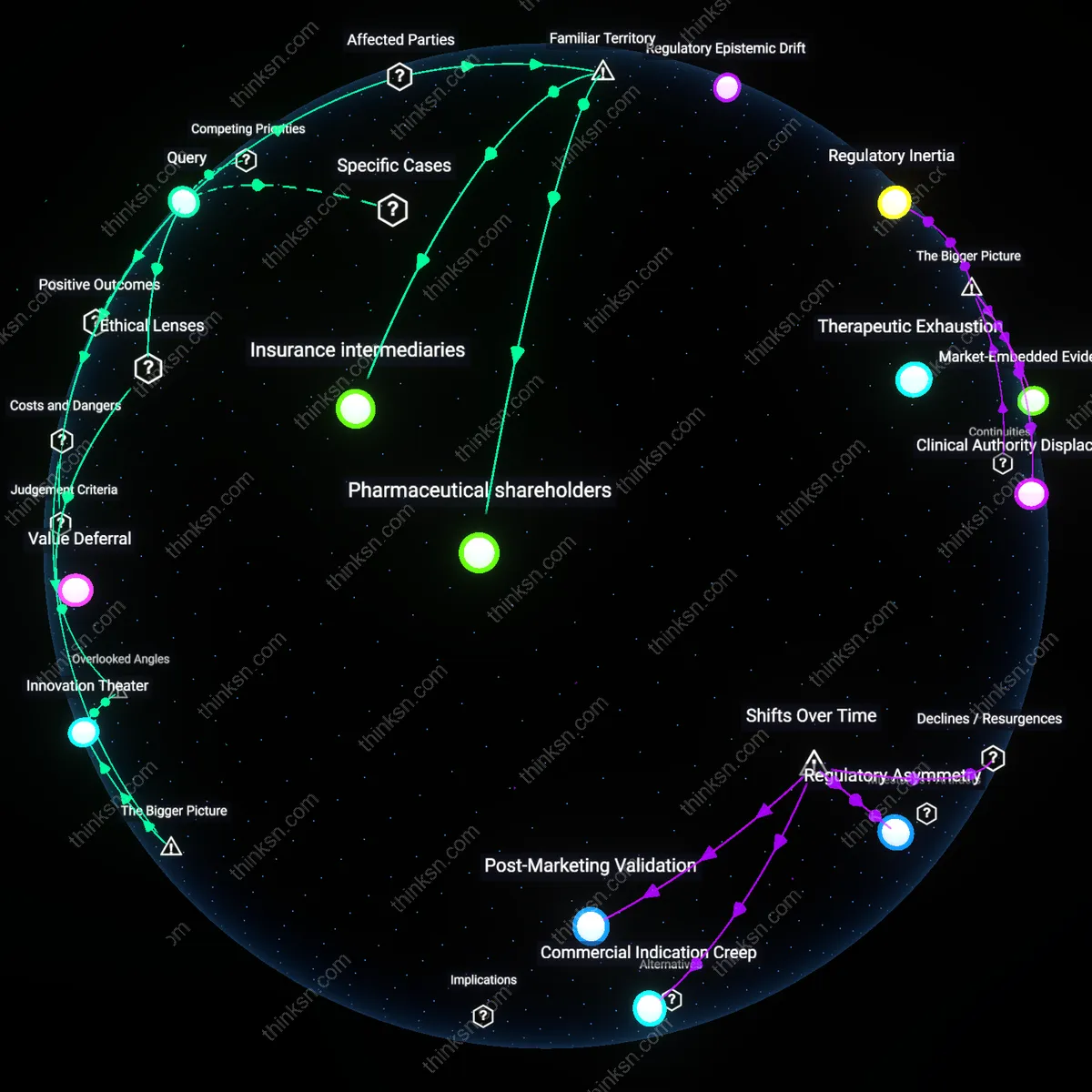
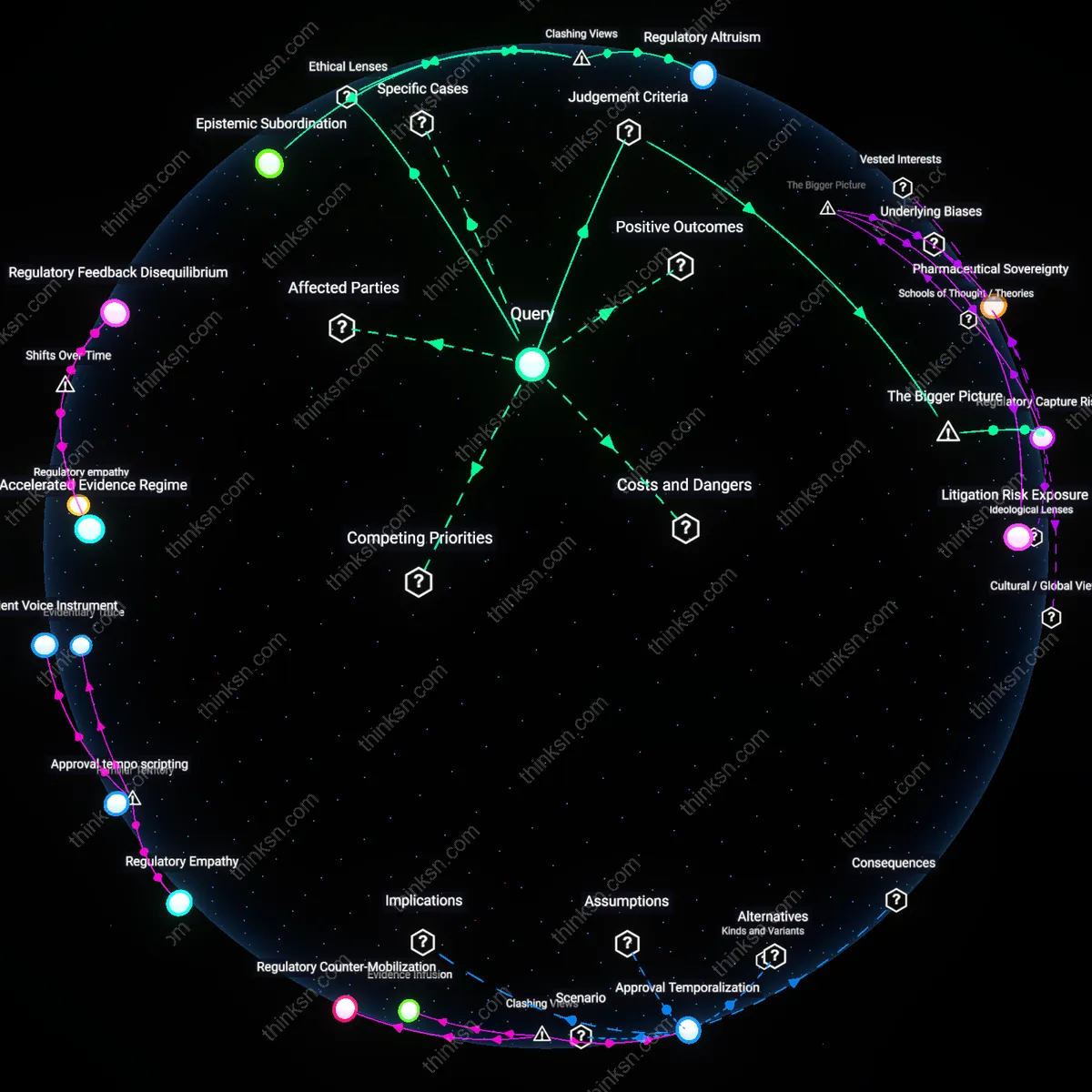
Therapeutic Exhaustion
The normalization of prescribing marginally effective drugs became entrenched when specialist communities, particularly in oncology and rare diseases, redefined therapeutic ambition downward in response to repeated failures in high-efficacy drug development—treating disease stabilization or minimal progression delay as success not because evidence demanded it, but because hope infrastructure required it. This pivot, visible in FDA’s accelerated approvals for drugs like bevacizumab and aducanumab, institutionalized a moral economy where attempting treatment became ethically mandatory, even when benefits were dwarfed by risks or costs. Against the dominant narrative of corporate or regulatory failure, the deeper driver is a medical culture unwilling to concede therapeutic limits, thus retrofitting approval systems to sustain the appearance of progress.
Regulatory Inertia
The practice of approving drugs with marginal benefits became routine because regulatory agencies adopted incremental risk tolerance over time, normalizing approvals based on statistical significance rather than clinical meaningfulness. The U.S. FDA’s acceptance of surrogate endpoints—like tumor shrinkage instead of survival or quality-of-life improvements—enabled approval pathways that deprioritized patient-relevant outcomes, particularly in oncology and chronic disease. This shift was institutionalized through mechanisms like accelerated approval and advisory committee influence, where evidentiary thresholds eroded not through policy reversal but through repeated exceptions that became precedent. What is underappreciated is that the agency’s credibility-preserving continuity—avoiding dramatic policy shifts—allowed gradual normalization of weaker evidence, making marginal benefit a systemic default.
Market-Embedded Evidence
Drug approval practices evolved to accept marginal benefits because pharmaceutical innovation became financially dependent on extending patent life through line extensions and reformulations that offered minimal therapeutic gain. Firms like AstraZeneca and AbbVie optimized clinical trial design to detect statistically significant but clinically trivial differences—such as dosing schedules or secondary endpoints—thereby generating approvable data without transformative effects. This is sustained by a feedback loop between payers, who reimburse on availability rather than value, and manufacturers, who align R&D with regulatory feasibility rather than unmet need. The underappreciated dynamic is that evidence production itself is shaped by return-on-investment calculations, making marginality not a failure of science but a market-calibrated outcome.
Clinical Authority Displacement
The routinization of prescribing marginally beneficial drugs emerged as clinical decision-making authority shifted from individual physicians to guideline bodies and formularies that rely on population-level trial data, often produced by industry. Professional organizations like the American College of Cardiology or NCCN incorporate drugs with small effect sizes into standards of care once they are FDA-approved, effectively endorsing marginal interventions as baseline therapy. This displacement occurs because guidelines prioritize consistency and legal defensibility over nuance in benefit interpretation, and because prescribers face greater liability for withholding approved treatments than for overtreating. The overlooked consequence is that clinical discretion is eroded not by corporate influence alone, but by systemic risk-aversion embedded in medical governance structures.
Regulatory Asymmetry
The routine approval of marginal-benefit drugs became entrenched after the 1992 Prescription Drug User Fee Act (PDUFA), which shifted the FDA’s performance metrics toward speed of review, creating a structural bias favoring approval over rigorous therapeutic scrutiny. Industry-funded user fees tied review timelines to sponsor payments, incentivizing efficiency in application processing while weakening the agency’s countervailing mandate to enforce clinical significance thresholds. This institutional reorientation—driven by biotech lobbying and AIDS activist demands for faster access—normalized non-curative endpoints like progression-free survival or biomarker shifts, allowing drugs with statistically detectable but clinically trivial effects to gain market authorization. The underappreciated consequence was not just faster approvals, but a recalibration of evidentiary standards that treated market entry as a right of submission rather than a privilege of demonstrated benefit.
Commercial Indication Creep
Pharmaceutical firms institutionalized marginal-benefit prescribing in the 2000s by repurposing failed or narrowly effective drugs into broader, less severe indications where competition was low and outcome measurement was forgiving. Blockbuster statins, initially developed for acute hypercholesterolem desperately under regulatory pressure to generate revenue, were incrementally repositioned into primary prevention cohorts with minimal cardiovascular risk. This expansion relied on surrogate endpoints like LDL reduction, divorced from hard morbidity or mortality outcomes, and leveraged direct-to-consumer advertising to medicalize risk itself. What is rarely acknowledged is that this cycle of indication broadening did not reflect therapeutic advancement but rather a strategic adaptation to saturated markets, turning mild efficacy into durable profitability through volume-driven prescribing.
Post-Marketing Validation
The normalization of marginal-benefit drugs accelerated after 2007’s FDA Amendments Act (FDAAA), which permitted conditional approval based on preliminary data, with confirmatory trials mandated only post-approval—a shift that inverted the evidentiary burden from pre-market proof to post-market verification. Oncology drugs, particularly in orphan indications, began routinely launching under accelerated pathways while confirmatory studies were delayed, underfunded, or quietly abandoned, allowing marginal efficacy to solidify as clinical standard. Payers, providers, and patients, once committed to treatment infrastructures, resisted de-approvals even when follow-up trials failed, as seen with agents like bevacizumab in breast cancer. The overlooked dynamic is that regulatory forgiveness became a predictable feature, embedding a de facto lifecycle where initial approval cemented market presence regardless of later disconfirmation.