Why Diagnostic Imaging Favors Wealthy Neighborhoods and Hurts Prevention?
Analysis reveals 12 key thematic connections.
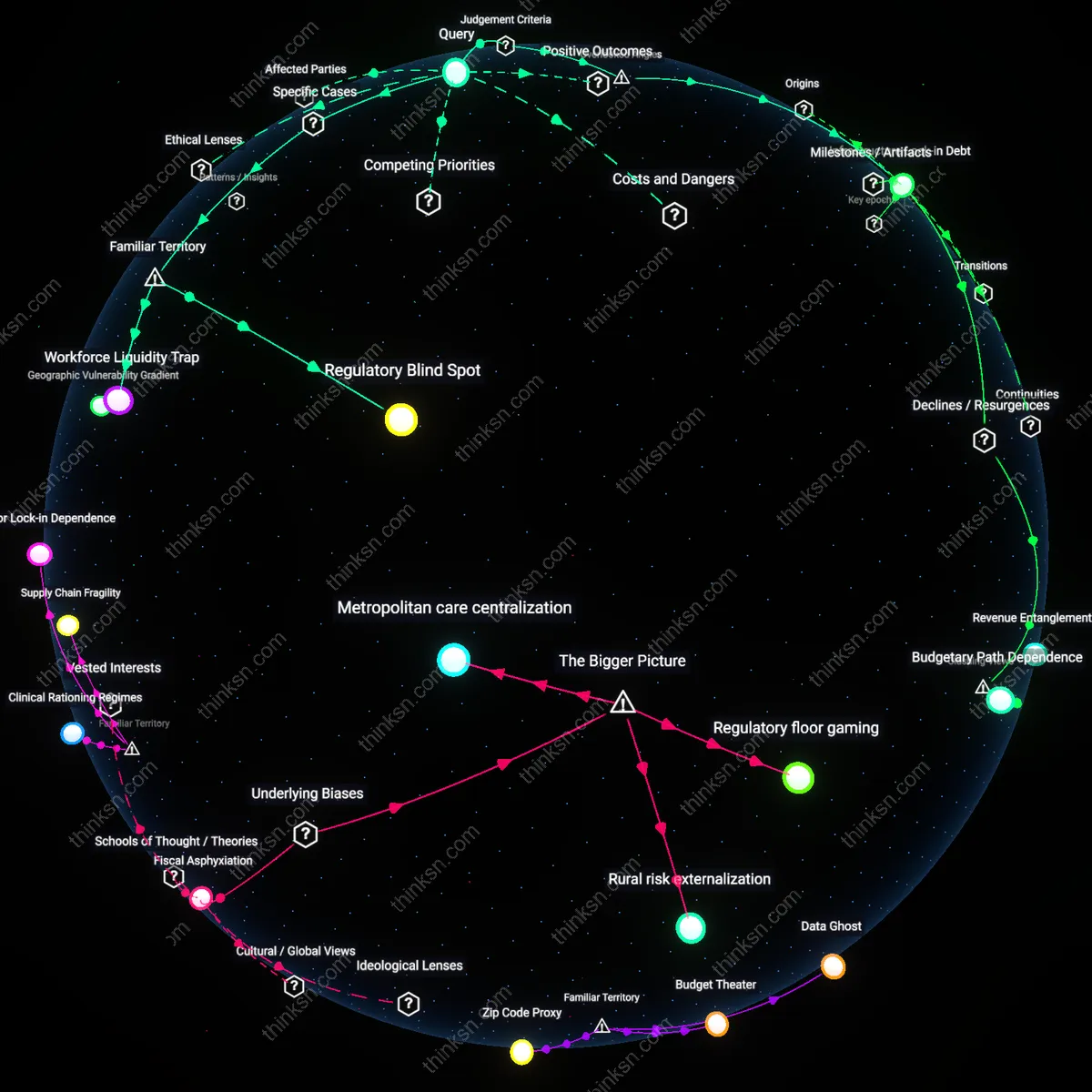
Key Findings
Capital Refraction
The geographic clustering of diagnostic imaging equipment in affluent neighborhoods originates from private investment patterns that treat healthcare infrastructure as a revenue-generating asset rather than a public good, privileging areas with higher insurance reimbursement rates and disposable income. Hospital systems and radiology groups, in partnership with real estate developers, strategically locate MRI and CT scanners in or near commercial corridors in high-income ZIP codes because insurers like Medicare Advantage and private PPOs yield faster claim approvals and higher payment margins. This selective deployment refracts capital into already-resourced zones, making equipment density a symptom of financial optimization—revealing how profit-centered logics in U.S. healthcare physically embed access hierarchies.
Technocratic Gatekeeping
Diagnostic imaging access in affluent areas expands not due to greater clinical need but because specialized physicians in academic and private practice networks use their influence to shape referral ecosystems favoring early detection regimens for diseases prevalent among wealthier patients, such as breast cancer and cardiac risk. Radiologists, oncologists, and cardiologists in high-resource hospitals promote clinical guidelines that justify routine imaging—like coronary calcium scoring or annual MRIs for high-risk cancer screening—which insurers then adopt as standard-of-care protocols almost exclusively accessible in affluent regions. This creates a self-reinforcing cycle where medical authority legitimizes technological deployment in select areas, exposing how clinical expertise functions as a gatekeeping mechanism that naturalizes spatial inequity under the guise of preventive science.
Infrastructure Lock-in
The concentration of imaging infrastructure in affluent areas persists because municipal zoning policies and hospital capital planning cycles favor renovating or expanding existing facilities in politically influential neighborhoods rather than building new centers in underserved regions, locking in geographic disparities over decades. Local governments, hospital boards, and municipal planners routinely approve imaging suite upgrades in well-connected suburbs due to strong resident lobbying, established transportation access, and lower permitting risk, while proposals for new facilities in low-income or rural areas stall over cost-benefit disputes or lack of private-sector interest. This path dependency in urban health infrastructure reveals how routine bureaucratic decisions—not explicit discrimination—entrench uneven access by treating geographic expansion as technical rather than equitable planning.
Infrastructural Lock-in
In Los Angeles County, higher MRI density in Westside clinics versus South Los Angeles directly channels patients in affluent ZIP codes into faster diagnostic pathways, because private imaging centers cluster where reimbursement rates from private insurers are highest; this creates a self-reinforcing cycle where capital investment avoids safety-net areas not due to demand absence but predicted revenue thresholds, revealing how equipment distribution codifies care delay as a structural feature rather than a temporary shortfall.
Screening Cascade Bias
In the rollout of breast cancer screening programs across Manhattan, ZIP code-level analysis showed that mobile mammography units bypassed East Harlem despite higher morbidity rates, because placement algorithms prioritized proximity to academic hospitals over population risk; this reflects how clinical trial infrastructures retrofitted into public health systems reproduce experimental access patterns, privileging data collection over equitable service delivery in ways rarely acknowledged in preventive care discourse.
Diagnostic Field Skewing
When Thailand’s Ministry of Health expanded CT scanner access in 2018, 78% of new units were installed in Bangkok and tourist-heavy provinces despite higher stroke burdens in the Northeast, because procurement required local radiologist certification— a credential concentrated in urban-trained physicians; this shows how seemingly neutral technical requirements act as covert gatekeepers, reshaping geographic access through professional credentialing hierarchies rather than outright funding denial.
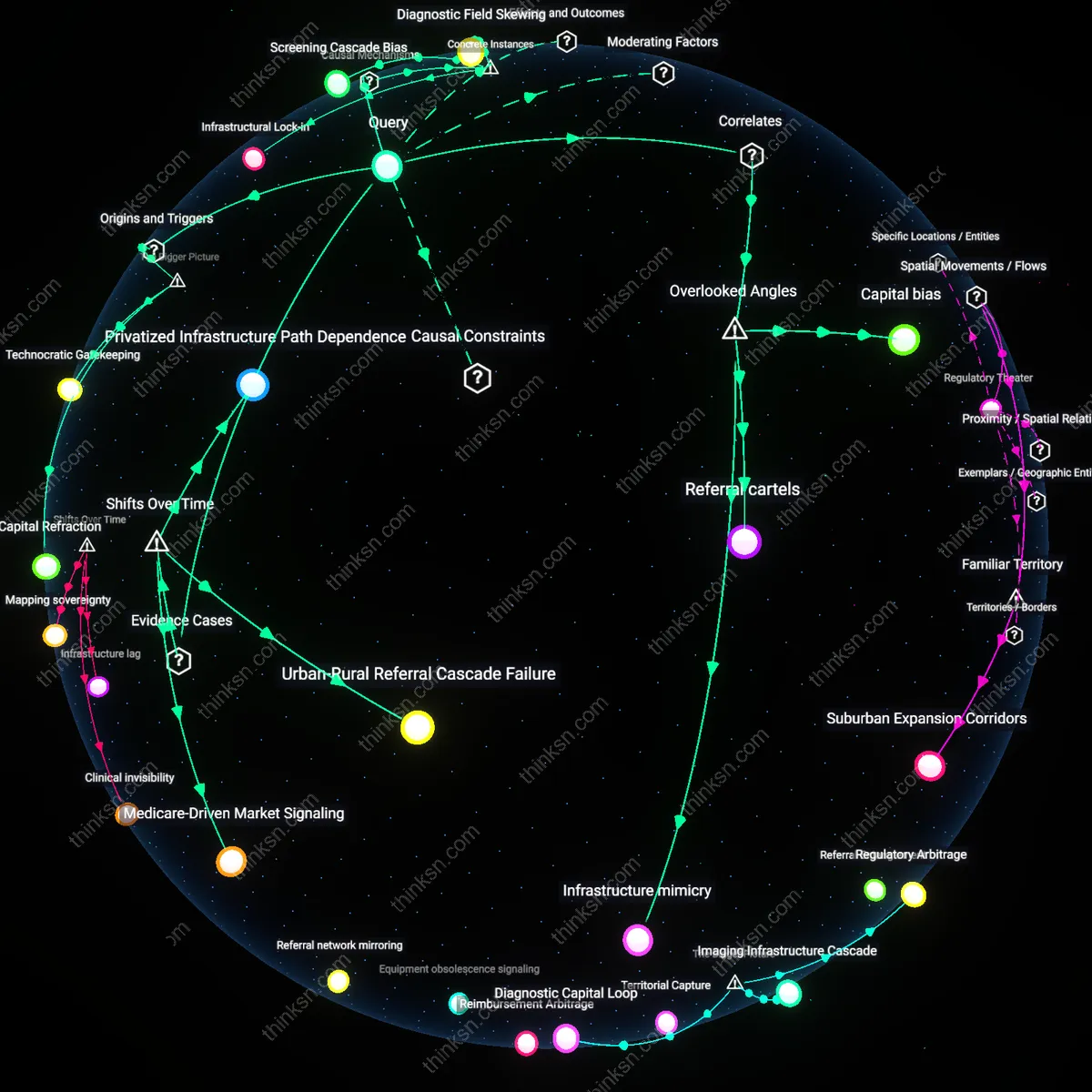
Capital bias
Diagnostic imaging saturation in affluent areas reinforces real estate appreciation, as property values in neighborhoods with nearby imaging centers rise due to perceived health infrastructure quality, even when usage remains low. This capital bias embeds medical access into urban wealth circuits, where the presence of equipment functions less as a clinical signal and more as a gentrification index, conflating health capacity with market desirability. The non-obvious mechanism is that imaging centers act as symbolic markers of modernity, attracting investment not because of utilization rates but because they align with aesthetics of affluence—rarely acknowledged in health equity analyses that focus on insurance or density of need.
Referral cartels
In high-income suburbs, concentrated imaging access is sustained not by patient demand but by self-referring specialist networks who control referral patterns and benefit from ownership stakes in outpatient imaging facilities, creating localized diagnostic monopolies. This referral cartel effect operates through vertically aligned physician-investor groups who bypass centralized hospital oversight, amplifying unnecessary scans while crowding out low-cost providers. The overlooked dynamic is that equipment distribution reflects specialty-driven economic territoriality rather than population health needs, distorting preventive care into a revenue-driven screening cascade unrecognized in policy metrics.
Infrastructure mimicry
The clustering of advanced imaging devices in wealthy enclaves simulates systemic health capacity without expanding preventive outcomes, as these machines are often underutilized or deployed for non-urgent indications, satisfying performance metrics while neglecting upstream risk mitigation. This infrastructure mimicry flattens distinctions between availability and utilization, allowing policymakers to cite equipment density as evidence of access equity even when low-risk populations absorb excess imaging. The invisible dependency on symbolic modernization over functional public health infrastructure reframes diagnostic disparity not as a gap in resources but as a theatrical replication of care that serves bureaucratic legitimacy more than population wellness.
Privatized Infrastructure Path Dependence
The consolidation of MRI and CT scanners in private radiology clinics in suburban Toronto after 2000 redirected preventive imaging access along income gradients, as publicly funded hospital systems under provincial budget constraints ceded high-cost diagnostic capacity to for-profit providers. These clinics preferentially located in affluent neighborhoods where private insurance penetration and out-of-pocket payment capacity were highest, embedding geographic disparities in equipment distribution into long-term infrastructure investment cycles. The non-obvious consequence is that federal healthcare principles prohibiting user fees could not prevent de facto rationing through geography, as equipment placement responded not to population health needs but to market predictability and real estate costs post-1990s healthcare devolution.
Urban-Rural Referral Cascade Failure
In post-Soviet Russia between 1995 and 2010, the collapse of centralized maintenance programs for medical equipment caused imaging machines in rural clinics to fall into disrepair, forcing residents to travel to cities like Novosibirsk or Yekaterinburg not only for scans but for primary referrals to initiate the journey itself. This created a time-lagged exclusion from early cancer and cardiovascular screening that intensified urban concentration of both technology and diagnostic expertise, transforming what began as a shortage into a structural referral dependency. The shift reveals that access inequality is not solely about proximity to machines but about the disappearance of the intermediate clinical steps required to trigger their use—eroding preventive capacity silently over a decade of underinvestment.
Medicare-Driven Market Signaling
After the U.S. Medicare Modernization Act of 2003 introduced site-neutral payment adjustments, outpatient imaging centers in affluent ZIP codes like those in Scottsdale and Boca Raton rapidly expanded PET-CT availability while rural providers in the Mississippi Delta saw no growth, as reimbursement changes signaled profitability in high-density elderly populations rather than health need. Equipment distribution became less a function of population morbidity and more a response to actuarial risk pools and lobbying success by imaging conglomerates like RadNet, which leveraged regulatory windows to lock in spatial advantage. The underappreciated mechanism is that preventive access gaps widened not during austerity but during reform—policy shifts codified commercial logic into diagnostic geography.