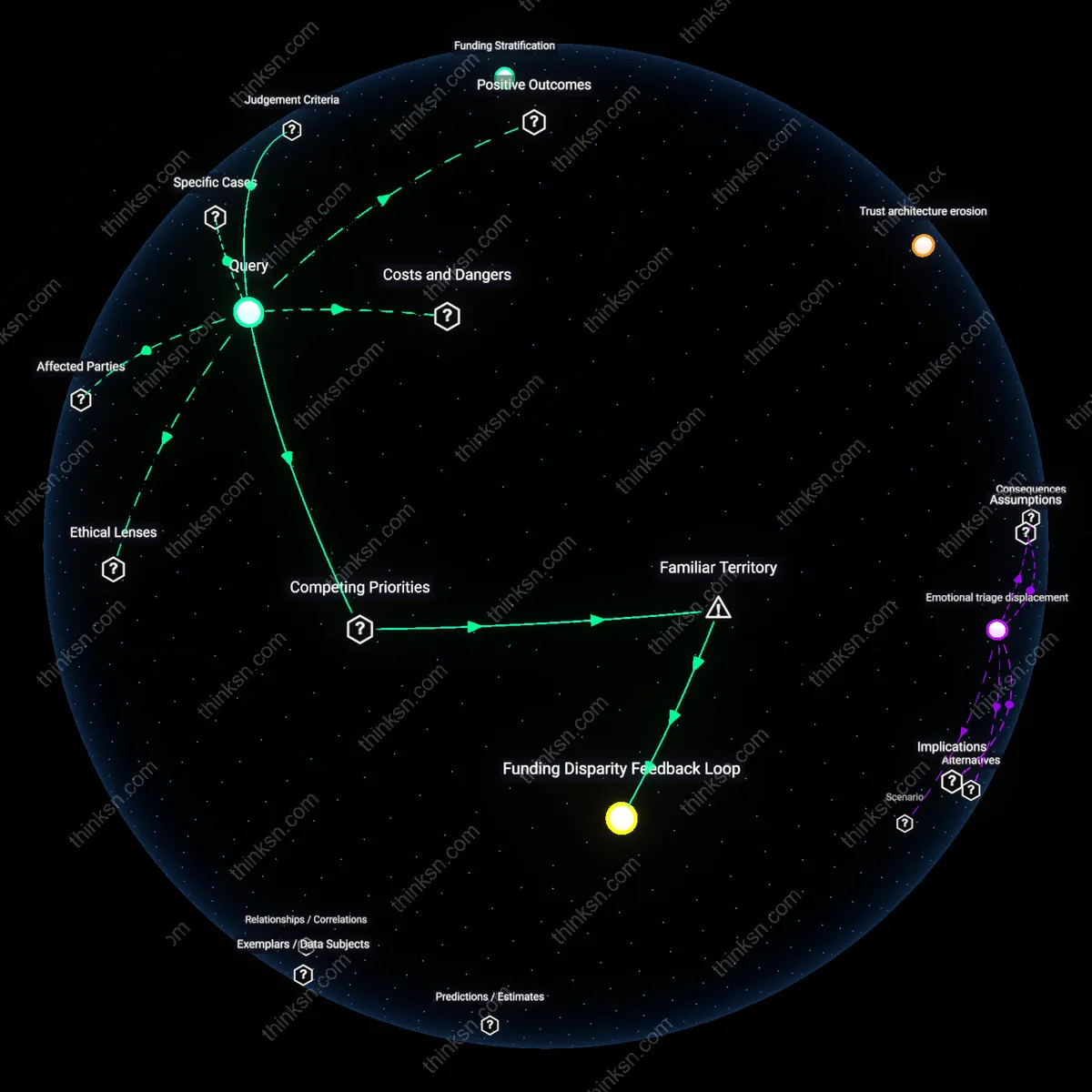
Mental Health or Jails: What Values are at Stake?
Analysis reveals 8 key thematic connections.
Key Findings
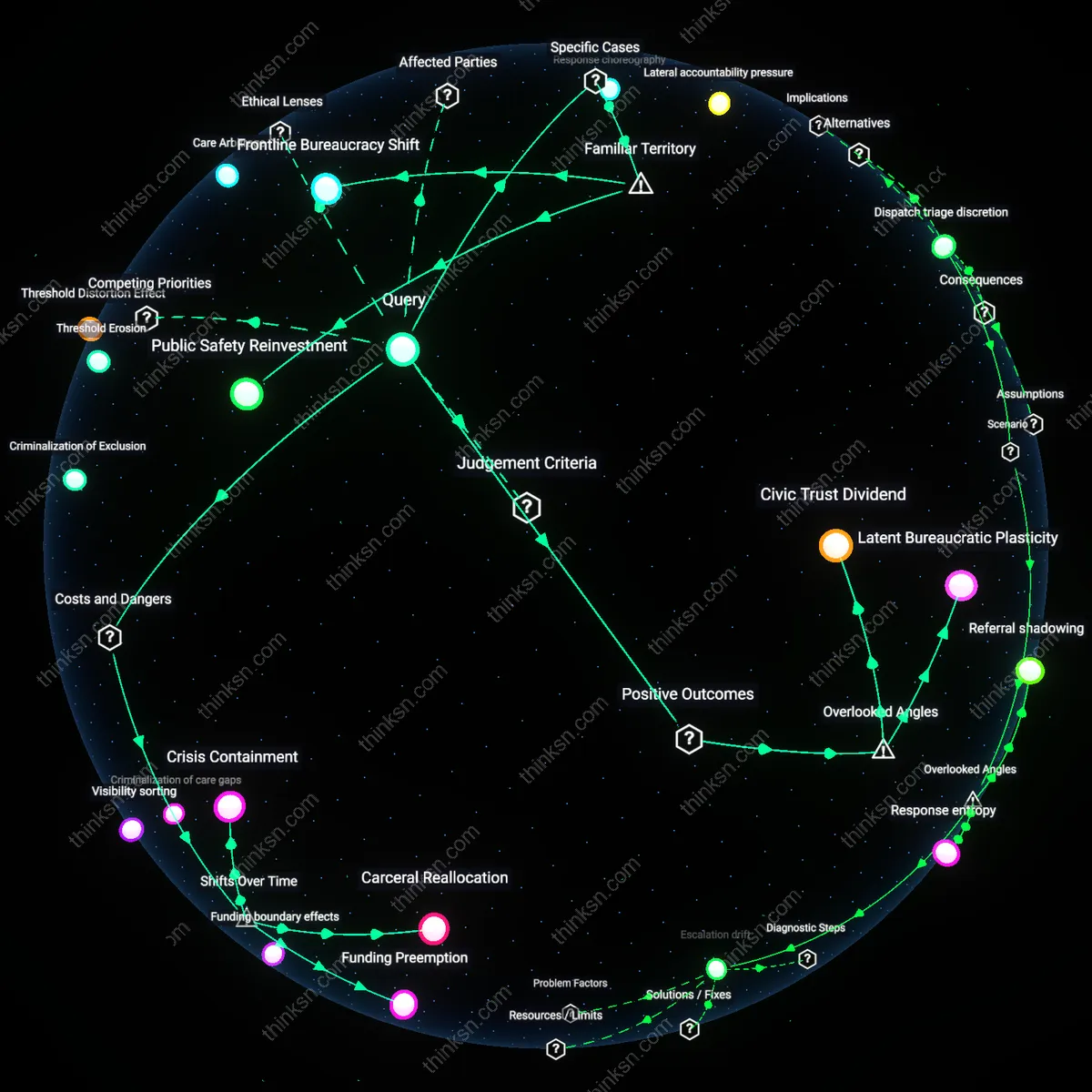
Civic Trust Dividend
Shifting funds from jail expansion to mental-health crisis teams strengthens neighborhood-level legitimacy of public safety institutions by replacing punitive visibility with relational response protocols. When unarmed clinicians resolve street-level behavioral crises—such as in Eugene, Oregon’s CAHOOTS program—residents, especially in historically over-policed communities, experience public institutions as responsive rather than intrusive, which incrementally rebuilds trust eroded by decades of enforcement-heavy approaches. This dynamic is overlooked because most cost-benefit analyses of mental-health interventions focus on hospitalization rates or police time saved, not institutional legitimacy as a cumulative civic asset that alters community cooperation with law enforcement and public health initiatives.
Latent Bureaucratic Plasticity
Prioritizing mental-health crisis teams over jail capacity activates dormant coordination pathways between public health and emergency response systems, revealing adaptability in inter-agency infrastructure that typically remains inert under siloed funding. For example, when cities like Denver redirected funds to the STAR program, emergency dispatch systems had to reconfigure triage logic, training materials, and data-sharing agreements between health departments and 911 centers—changes that create modular templates for future cross-sector responses to housing instability or substance use. This institutional flexibility is rarely acknowledged because policy evaluations emphasize service outputs, not the evolving procedural architecture that determines how easily cities can pivot in future crises.
Moral Infrastructure Reservoir
Investing in mental-health crisis response cultivates a form of communal moral infrastructure—shared expectations that care, not containment, is society’s default response to distress—thereby shifting the ethical baseline of public responsibility. When non-violent behavioral incidents are met with clinicians instead of cells, as seen in crisis systems in San Francisco’s Mental Health SF program, community members, including bystanders and small business owners, begin to internalize and replicate de-escalatory norms, effectively expanding the reach of the intervention beyond funded staff. This reservoir of internalized ethics is typically absent from discussions that treat funding choices as zero-sum material tradeoffs, ignoring how institutional choices shape the moral cognition of ordinary residents over time.
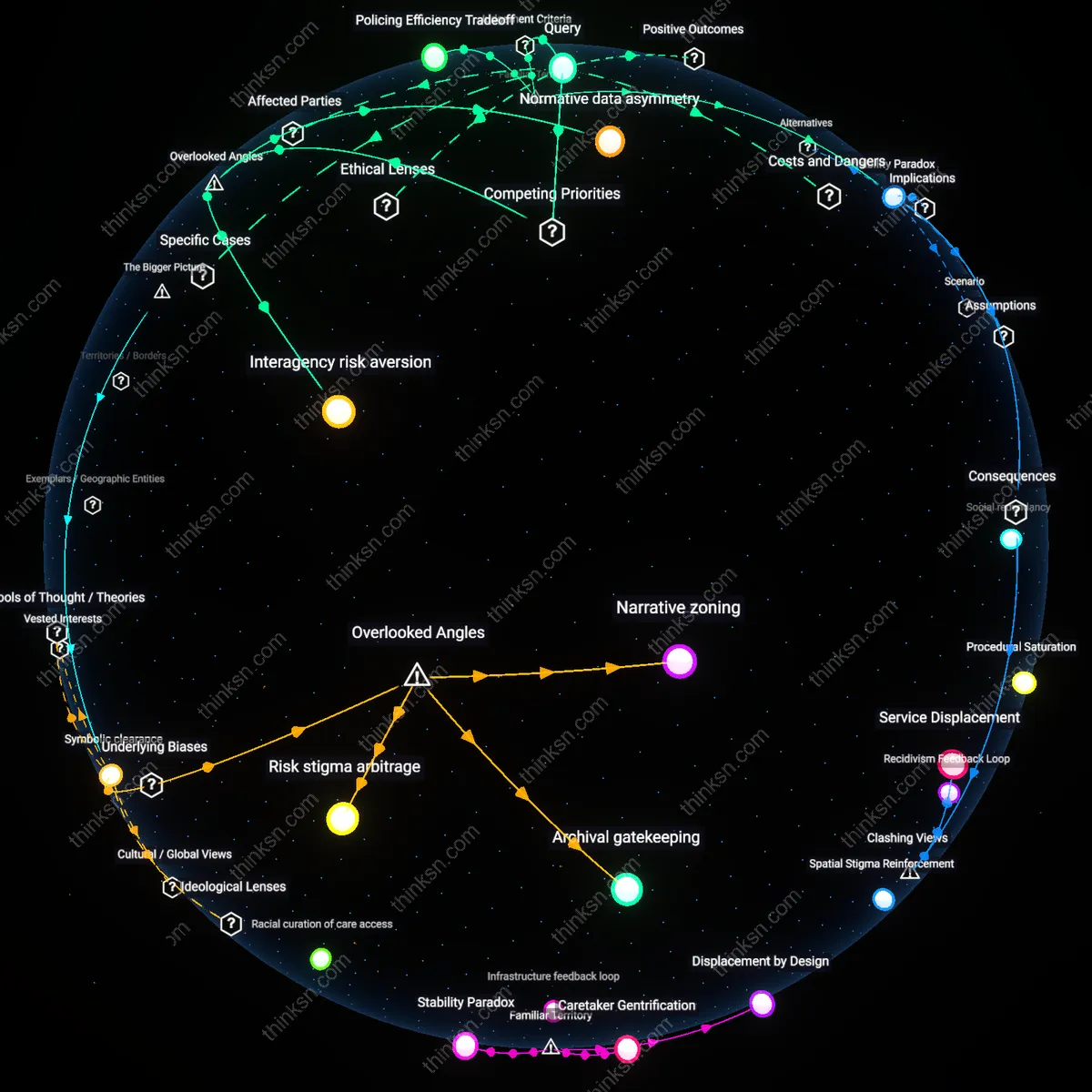
Carceral Reallocation
Diverting funds from jail expansion to mental-health crisis teams since the 1980s deinstitutionalization era has systematically transferred responsibility for social control from clinical to law enforcement domains, then back toward medicalized oversight—only now embedded within policing infrastructures. This reallocation does not dismantle carceral logic but repurposes it, using public health rhetoric to justify expanded surveillance of marginalized populations under the guise of care, particularly in cities like Los Angeles and Denver where crisis teams operate under police departments. The non-obvious consequence is that mental health interventions become contingent on threat assessment protocols developed for criminal behavior, reinforcing rather than reducing coercive state power.
Funding Preemption
The shift from jail expansion to crisis teams after the 2008 recession created a fiscal mechanism where mental health funding is only politically viable when it offsets corrections budgets, tying public health viability to penal growth projections. This linkage, evident in county budget hearings across Maricopa County and Cook County, means that mental health services expand only insofar as they prevent incarceration, not according to therapeutic need, thus preempting more holistic models like community clinics or housing-first programs. The underappreciated risk is that economic crises become catalysts for conditional care systems, where the value of a life is calculated by its potential cost to the jail system rather than its human dignity.
Crisis Containment
Following the 2020 racial justice uprisings, cities adopted crisis response teams as alternatives to policing—but this transition reframed mental distress as a public order issue requiring rapid stabilization, not long-term healing, privileging immediate de-escalation over sustained care. In Minneapolis and Portland, where crisis teams were implemented to reduce police use-of-force incidents, the model evolved to mirror emergency medicine rather than preventative health, creating a new tier of triage professionals trained to suppress volatility rather than address root causes. The overlooked danger is that this trajectory institutionalizes crisis as the only legitimate entry point into care, normalizing episodic intervention while eroding support for continuous, community-based mental wellness.
Public Safety Reinvestment
Shifting funds from jail expansion to mental-health crisis teams in cities like Denver directly redefines public safety to prioritize care over custody. Programs such as the STAR Initiative deploy health professionals instead of police to non-violent behavioral emergencies, reducing criminalization of mental illness by rerouting response through medical frameworks. The non-obvious insight is that this shift doesn’t just save money—it reconstitutes what institutions count as a threat, replacing penal logic with therapeutic triage in everyday urban governance.
Frontline Bureaucracy Shift
In Minneapolis, the replacement of police with mental-health clinicians on 911 mental health calls reassigns frontline authority from law enforcement to care providers, changing how state power is exercised in real time. This shifts discretion to clinicians to determine whether a situation requires intervention or de-escalation, embedding therapeutic judgment into emergency response protocols. What’s rarely acknowledged is that this subtly redistributes institutional legitimacy—credibility in crisis now flows to counselors, not cuffs, altering public perceptions of who 'keeps order.'