Do Diversion Programs for Drug Offenses Help or Harm Communities?
Analysis reveals 11 key thematic connections.
Key Findings
Justice Temporality
Diversion programs should be assessed by their reallocation of moral responsibility from punitive to rehabilitative institutions, marking a shift from late 20th-century criminalization to 21st-century therapeutic governance. This transition, visible in U.S. policy after the 2009 Obama-era Drug Policy Initiative, reframed drug use as a public health issue rather than a justice violation, transferring authority from courts to clinics and treatment providers. The mechanism—the substitution of probation-for-treatment agreements for incarceration—embeds a rehabilitative ideal that presumes moral malleability, making justice itself a time-bound process of reform rather than a moment of punishment. The underappreciated insight is that justice is no longer measured by sanction severity but by the duration and compliance demands of treatment trajectories.
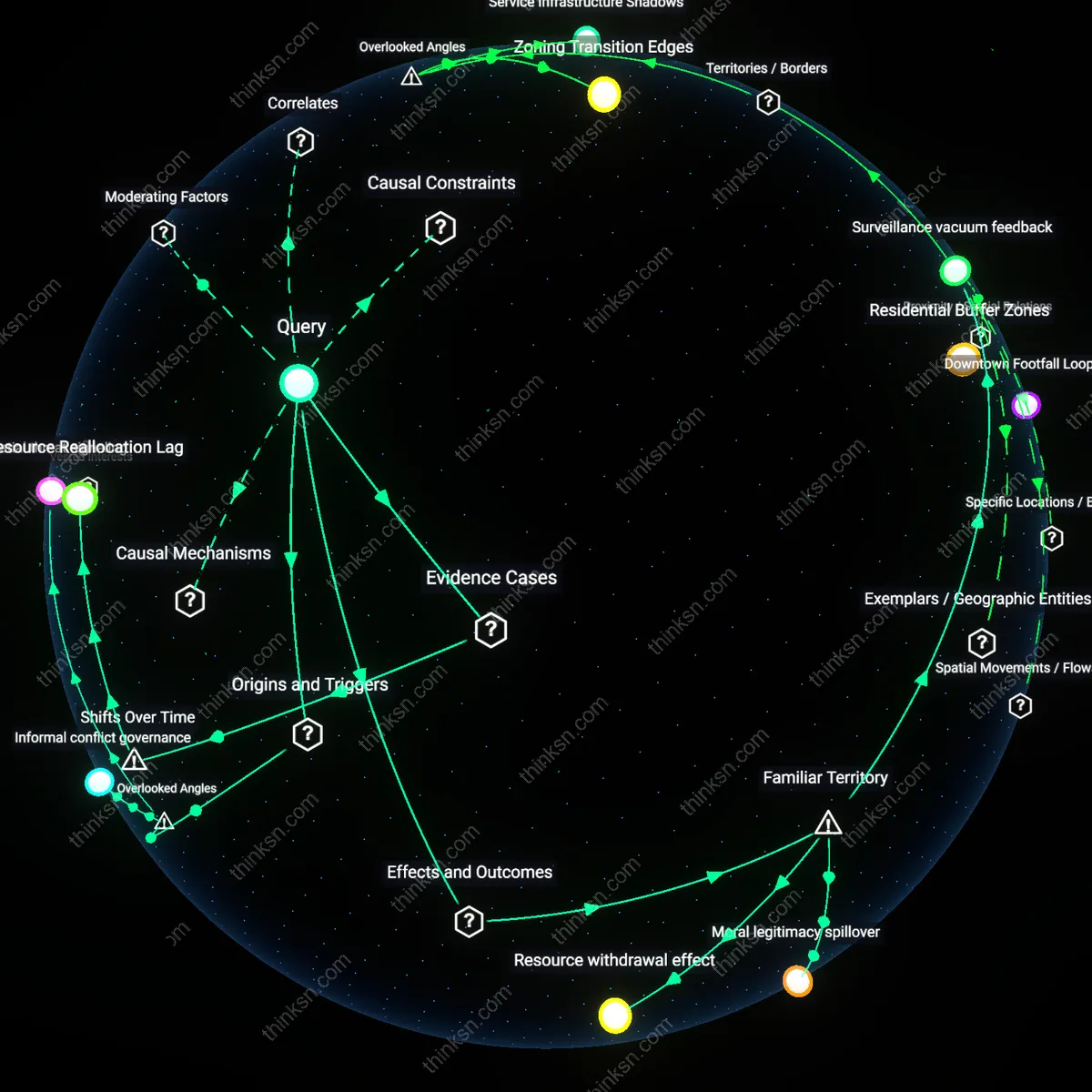
Market Feedback Lag
The effects of diversion on drug availability must be assessed through the delay between reduced enforcement pressure and downstream market restructuring, a dynamic revealed during the early 2010s as prescription opioid diversion outpaced supply controls. When law enforcement shifted focus from low-level possessors to trafficking nodes—evident in DEA scheduling changes and state PDMP rollouts—the unintended consequence was a temporary expansion of informal networks supplying diverted pharmaceuticals. This lag, where demand persists despite disrupted supply chains, caused a paradoxical spike in availability before adaptation, exposing how enforcement shocks propagate non-linearly through illicit circuits. The overlooked reality is that diversion programs alter enforcement patterns asymmetrically, creating temporal vacuums that traffickers exploit faster than public health interventions can fill.
Autonomy Assemblage
Community health outcomes of diversion programs should be judged by whether they expand individual capacity to act on health decisions, a shift institutionalized in post-2010 harm reduction cities like Seattle or Providence that integrated naloxone access with user-led education. The pivot from abstinence mandates to choice-based models—seen in Rhode Island’s peer-navigated recovery programs—activates autonomy not as abstract right but as a networked effect of syringe exchanges, supervised consumption, and housing-first policies. These systems treat agency as emergent from material supports, not personal willpower, making health gains dependent on whether services co-locate rather than refer. The unnoticed transformation is that autonomy now functions as a technically sustained configuration, not a moral precondition for care.
Reduced Overdose Clusters
Diversion programs improve community health by linking first-time drug offenders to treatment instead of jail, which increases access to naloxone and counseling in high-risk neighborhoods like those in rural Ohio or inner-city Baltimore. Public health workers use these programs as entry points to disrupt opioid transmission chains through coordinated outreach, effectively turning criminal justice touchpoints into public health interventions. The non-obvious shift is that law enforcement becomes a referral mechanism rather than a barrier, counter to the popular image of police as purely punitive actors in drug cases.
Street Market Displacement
Diversion programs indirectly reduce local drug availability by shrinking the pool of low-level dealers who enter or re-enter the market after incarceration, a pattern visible in cities like Seattle where repeat petty offenders no longer cycle through jails and back into street economies. Courts funnel participants into job training or education, removing them from survival-based distribution roles often tied to neighborhood open-air markets. The overlooked dynamic is that decarceration disrupts informal recruitment pipelines, a function rarely attributed to health-focused justice reforms in public debate.
Community Trust Infrastructure
Diversion programs strengthen public health outcomes by building sustained trust between residents and institutions in over-policed areas such as the South Bronx or East Oakland, where participation in treatment is more likely when perceived as voluntary rather than coerced. Health departments leverage consistent contact with diverted individuals to map emerging drug use trends and deploy mobile clinics proactively. What’s underappreciated is that the reduction in legal stigma generates reliable health data streams—something traditional enforcement suppresses by driving use underground.
Pharmaceutical Supply Chain Feedback
Diversion programs reduce arrest-based seizures of small-scale drug operators, inadvertently altering procurement patterns among wholesale distributors who recalibrate routes based on expected interdiction levels. Because law enforcement seizures feed into pharmaceutical supply risk models—used by legitimate and illicit distributors alike—lower confiscation volumes signal reduced operational risk, encouraging faster transit and expanded distribution networks. This feedback loop is rarely accounted for in public health assessments, which focus on individual behavior change rather than market-level signal transmission through interdiction data. The overlooked mechanism is how enforcement metrics, even when declined for rehabilitative goals, function as market intelligence that modulates drug availability.
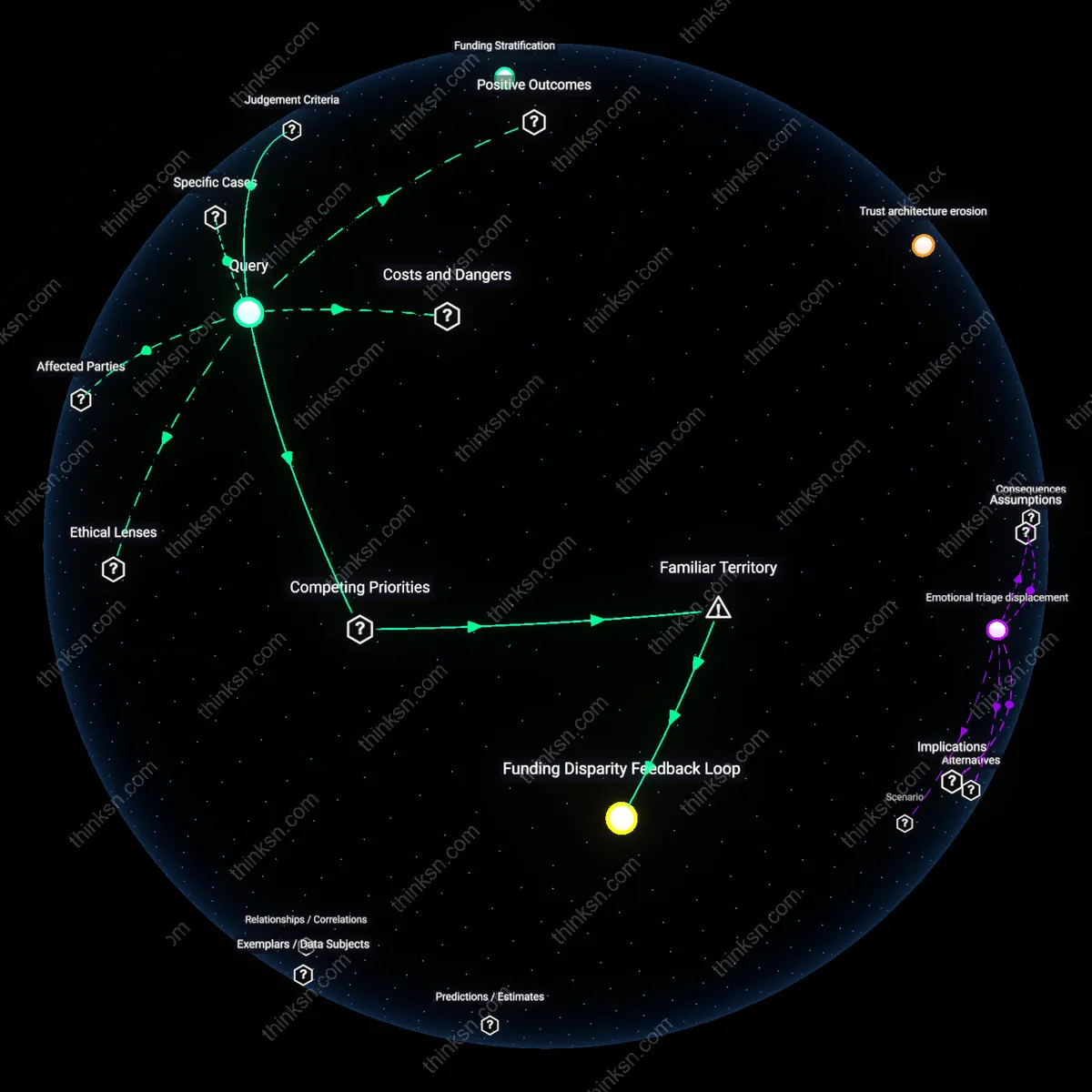
Civic Trust Arbitrage
Communities with high participation in drug diversion programs experience improved trust between residents and local health authorities, but this same trust is exploited by informal drug networks that co-opt program-associated spaces—such as harm reduction centers—for stealth distribution under the cover of medical legitimacy. Because these venues gain social legitimacy and reduced police scrutiny, they become high-value territories for discreet drug reallocation, particularly for substances like diverted pharmaceuticals or fentanyl analogs. The non-obvious tradeoff is that the very trust essential for health outreach becomes a currency for illicit actors to minimize detection, shifting drug availability into semi-medicalized zones where monitoring is politically sensitive.
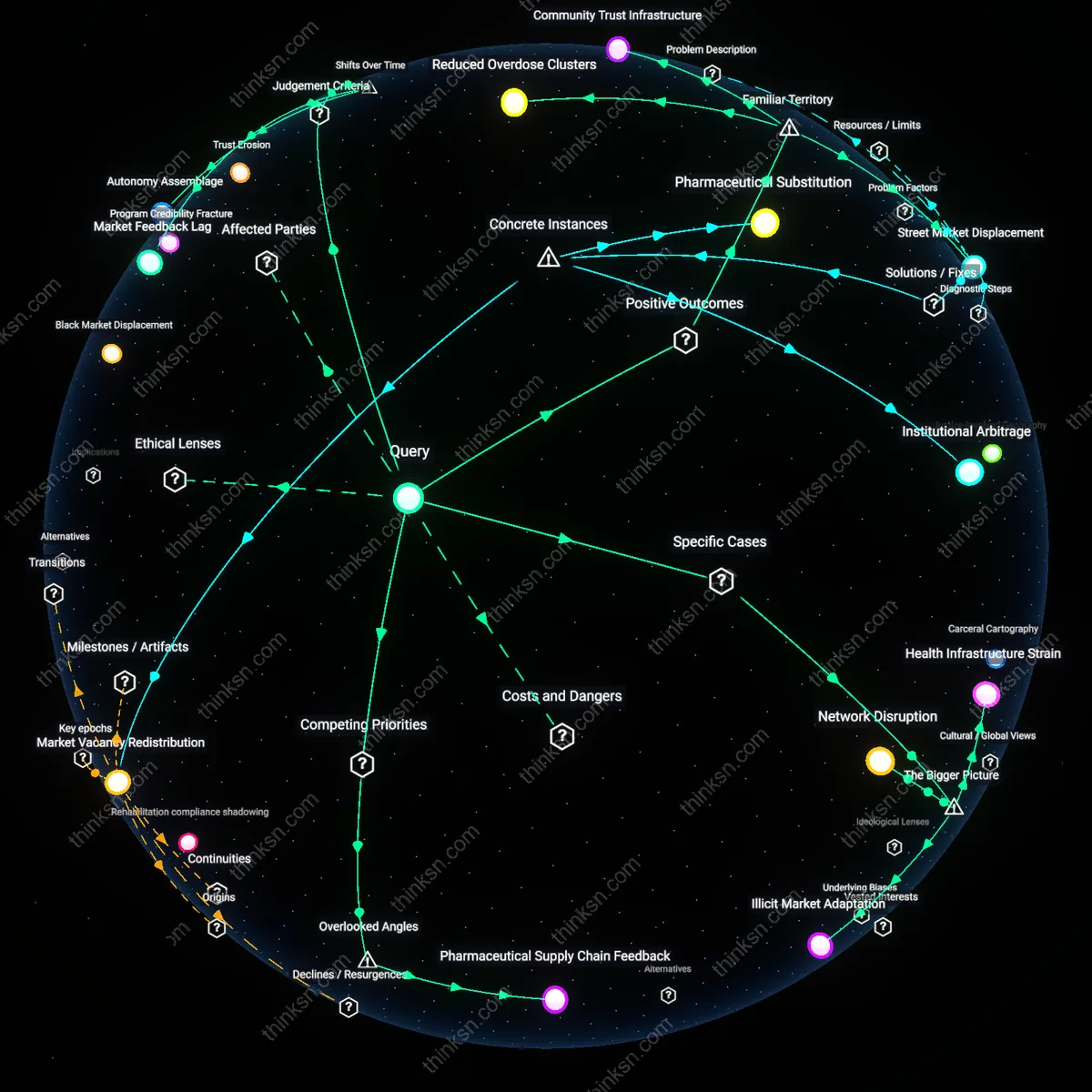
Network Disruption
Diversion programs in King County, Washington reduce drug availability by redirecting low-level offenders from incarceration to health-based interventions, thereby weakening nonviolent participants’ integration into trafficking networks. Prosecutors and public health officials collaborate to identify eligible defendants, whose removal from street-level distribution roles—often driven by addiction and economic precarity—fractures localized supply chains more effectively than incarceration, which tends to compress and strengthen such networks through prison-based ties. This dynamic reveals that the systemic effect of diversion is not merely harm reduction but a form of indirect market destabilization, a mechanism often overlooked in evaluations focused solely on recidivism or treatment uptake.
Health Infrastructure Strain
In Baltimore, Maryland, the expansion of drug diversion programs without proportional investment in community health capacity has shifted untreated demand into overstretched public clinics, increasing strain on frontline providers and displacing resources from chronic disease care. As courts refer more individuals to counseling and monitoring services, the city’s federally qualified health centers—already operating at capacity—face triage-level decisions about service delivery, illustrating how judicial policy changes act as a transfer mechanism of public risk into under-resourced health systems. This exposure of infrastructural fragility underscores that the success of diversion is not solely determined by program design but by the absorptive capacity of the public health ecosystem it feeds into.
Illicit Market Adaptation
In rural counties of Kentucky, where opioid diversion programs have expanded under state-funded treatment initiatives, local cartels have responded by lowering prices and increasing purity to stimulate addiction-driven loyalty, effectively countering reduced street-level trafficking due to decriminalization. This market elasticity is enabled by the decentralized nature of fentanyl supply chains and weak interdiction capacity, allowing distributors to bypass traditional hierarchies and rely on social networks rather than coerced labor. The result is a paradox where community health interventions aimed at reducing drug-related harm inadvertently stabilize demand, revealing how illicit economies co-opt public health progress when enforcement and supply-side disruption remain uncoordinated.