Is Referring for Abortion Across State Lines Illegal?
Analysis reveals 6 key thematic connections.
Key Findings
Medical Shielding
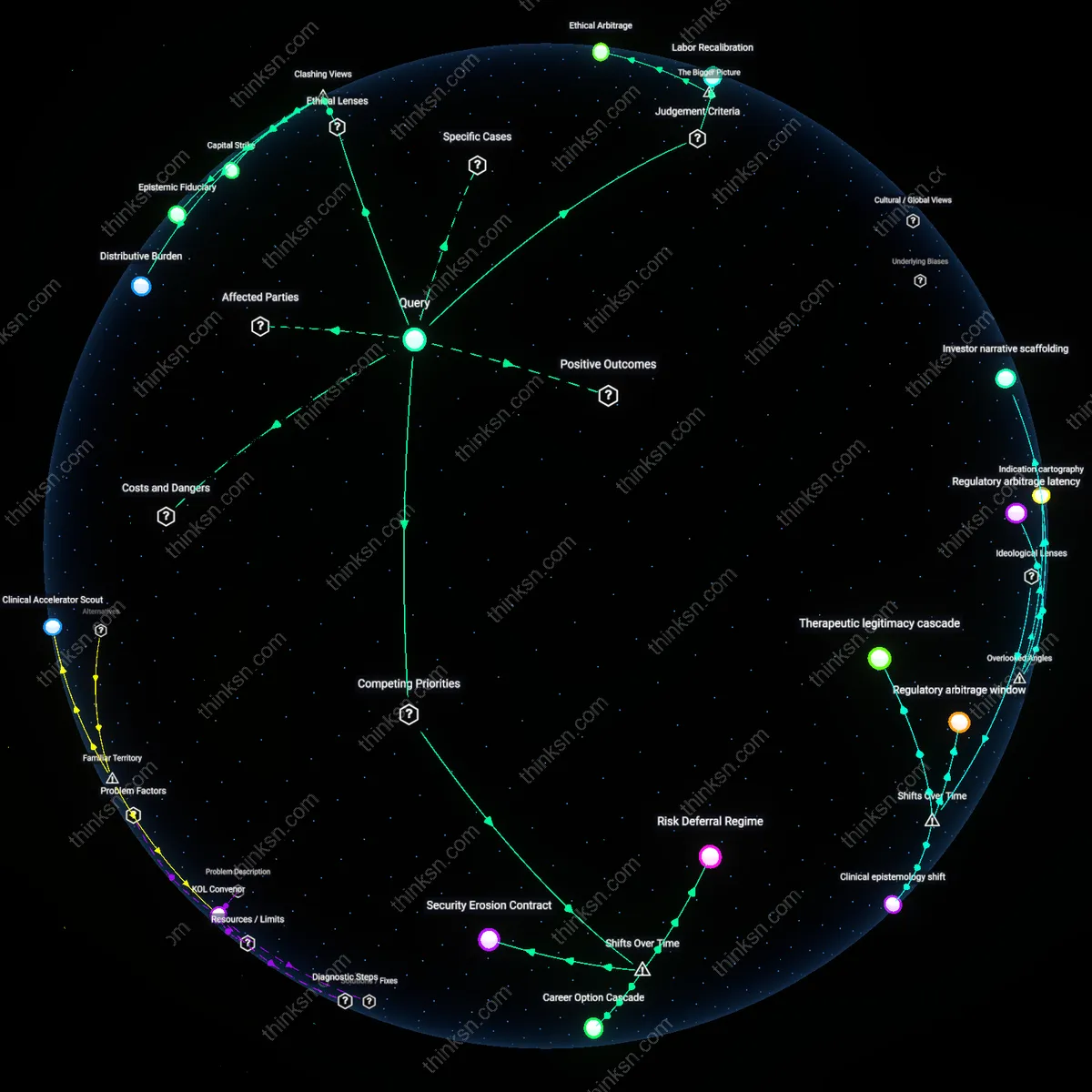
A physician’s referral for an abortion across state lines can be criminalized when states extend liability to facilitators, as in Texas under SB 8, where civil enforcement enables private citizens to sue anyone aiding an abortion, including referring physicians, thereby transforming medical guidance into a legally punishable act through third-party enforcement. This mechanism, deployed in Texas after the 2021 enactment of Senate Bill 8, dissuades physicians from providing referrals even when technically out of state because the law attaches liability to any actionable assistance, revealing the strategic use of civil enforcement to deter medical support networks across borders and collapsing the distinction between care and complicity.
Jurisdictional Overreach
In Idaho, following the state’s 2022 abortion trigger ban and subsequent court battles over emergency exceptions, physicians referring patients out of state faced potential investigation by state medical boards under rules interpreting referral as participation in a prohibited act, illustrating how restrictive jurisdictions legally construe cross-border medical referrals as conspiratorial conduct under medical licensure frameworks. The case of Dr. Cassandra Sparks, who was questioned by Idaho’s Board of Medicine for referring a pregnant patient to Oregon, revealed that the state treated referral as de facto facilitation, thus stretching the reach of local criminal norms into extraterritorial medical advice through professional oversight mechanisms, a non-obvious extension of sovereignty into inter-state medical practice.
Clinical Displacement Risk
After Mississippi’s Gestational Age Act took effect in 2022, physicians at University Women’s Health Clinic in Jackson reported self-censorship in discussing out-of-state abortion options, fearing that documented referrals could be interpreted as evidence of intent under broad conspiracy statutes inherited from pre-Roe legal frameworks, exposing how legacy laws originally designed to enforce total abortion bans resurface to criminalize medical speech. This demonstrates how physicians’ evolving triage decisions under threat of prosecution lead to the erosion of standard care pathways, not due to explicit legislation on referrals, but because indirect legal tools amplify perceived risk, making ordinary clinical judgment a target for retroactive criminalization.
Legal Shield Erosion
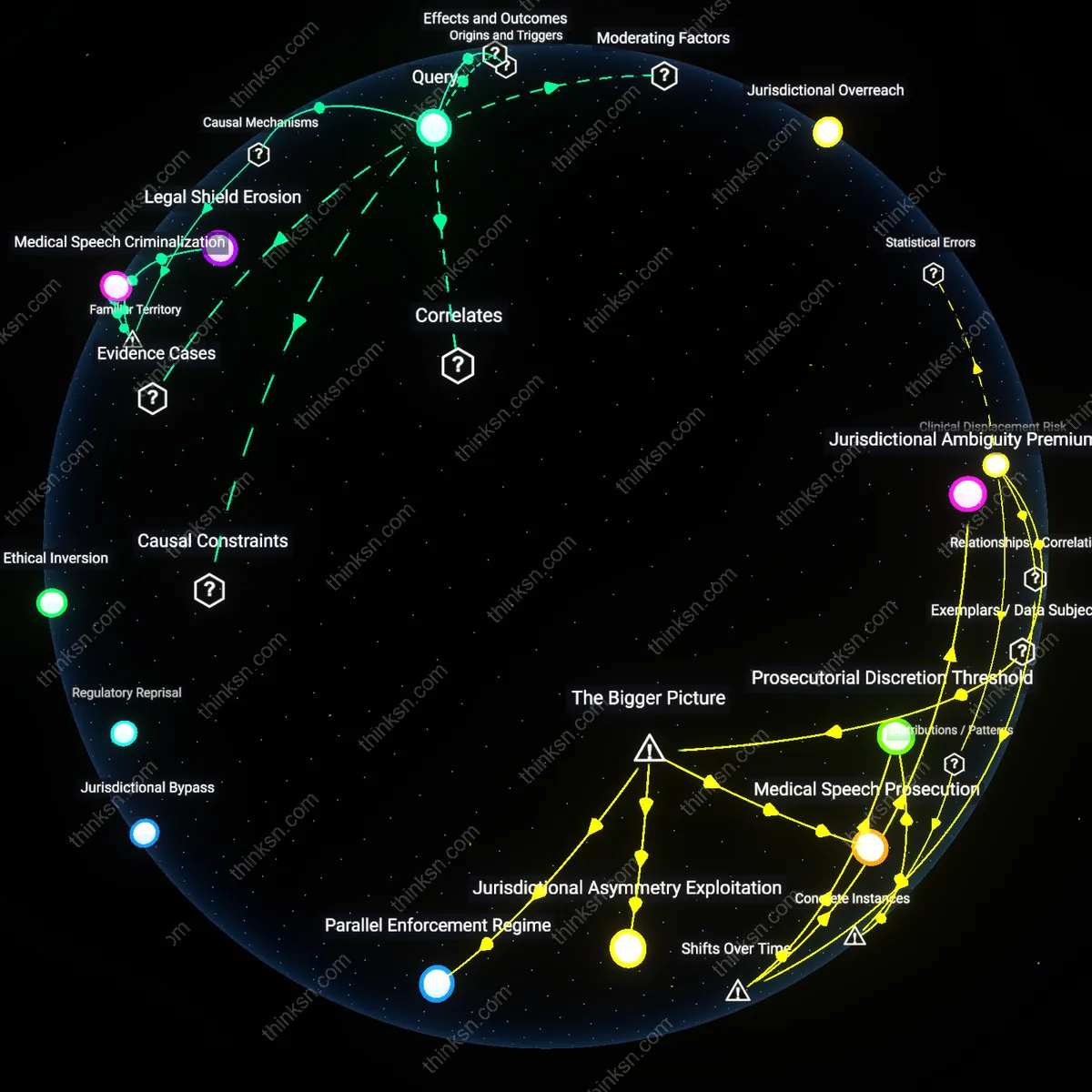
A physician’s referral for an abortion across state lines can be prosecuted in restrictive jurisdictions because state laws may interpret the referral as conspiracy to commit abortion, triggering criminal liability under complicity doctrines. This occurs when prosecutors apply aiding-and-abetting statutes to medical guidance, transforming advice into actionable facilitation within a jurisdiction that criminalizes the outcome. The mechanism relies on extraterritorial enforcement of state criminal law, where intent and proximate cause are legally imputed across borders, making the act of referral—typically protected medical speech—vulnerable to reclassification as criminal conduct. What is underappreciated is that even without performing the procedure, the physician’s role becomes legally indistinct from direct participation under these interpretive frameworks.
Medical Speech Criminalization
A physician’s referral can become a criminal act in restrictive states because giving medical advice that enables access to out-of-state abortion care may be redefined as unlawful speech under public policy exceptions to professional autonomy. This shift happens when state legislatures pass laws that designate certain medical referrals as unprotected speech if they relate to procedures deemed illegal in-state, thereby activating legal penalties through licensing boards or criminal codes. The causal pathway runs from legislative definition to regulatory enforcement, where medical communication loses its shield once it is framed as instrumental to violating state moral statutes. The overlooked reality is that clinical judgment, traditionally insulated, becomes prosecutable when speech is legally fused with downstream effects.
Jurisdictional Contagion
A referral can be criminalized in restrictive states because legal authorities assert jurisdiction over the intent behind medical actions, not just the location of the procedure, effectively extending territorial law into networked medical practice. This operates through legal theories that treat cross-state referrals as in-state offenses when the physician is state-licensed and the patient is state-resident, allowing prosecutors to anchor criminal jurisdiction in professional licensure rather than geography. The mechanism depends on states weaponizing medical board oversight to enforce moral statutes beyond their borders, converting administrative authority into penal reach. What’s rarely acknowledged is that licensure—a tool of professional regulation—becomes a vector for criminalization when detached from clinical ethics and repurposed as a legal boundary.